

Reading Between the Lines, Bibliotherapy
Have you ever heard of bibliotherapy? I’m always trying to identify ways to start working on recovery from depression, but I never thought much about one of the first steps I took – reading. I was surprised to learn that reading books for medical treatment dates to World War II, when it proved effective for wounded veterans. Bibliotherapy also seems to be helpful for depression.
Even though I first learned that “depression” was the name for my problems when I was in my twenties, a couple of decades went by before I really studied the disorder. That may seem odd since I’d been in therapy on and off for many years and had also taken a number of antidepressants. I think the delay in trying to learn more was one sign of my resistance to treatment as well as a denial of how seriously depression was affecting my life. Besides that, neither psychotherapy nor medication had helped me for very long.
Something was missing, and reading about how I could help myself opened new possibilities. It was like the healing effect of writing. There was something about getting new concepts and ideas into my mind, as well as down on paper, that made an enormous difference. These activities helped me get a real start on recovery.
Feeling Good
There are claims that reading self-help books on depression may be do more than get you started. There is some evidence that it may also work as the primary therapy for major depressive disorder. I find that a bit far-fetched. Even if I could have read all the thousands of self-help books on depression, that activity alone would never have dealt with the severe illness I lived with. Apparently, though, working with the best self-help books can work for people with mild to moderate depression.
If you’re familiar with David Burns’ classic Feeling Good: The New Mood Therapy, you can read in the introduction about formal studies on the therapeutic effectiveness of reading self-help books – specifically that one.
In the study Burns discusses, about 75% of the participants no longer met the criteria for a major depressive episode after four weeks spent reading his book – using no other therapy. All had met the criteria for major depressive disorder (not just a single episode) going into the study. That rate of recovery is impressive, even though it was clear that those with severe depression needed additional help. But did recovery hold up over time? To answer that question, the participants were interviewed and tested again after three years.
The diagnostic findings at the three-year evaluation confirmed [earlier improvement] — 72% of the patients still did not meet the criteria for a major depressive episode and 70 percent did not seek or receive any further treatment with medications or psychotherapy during the follow-up period. … While it is encouraging that many patients seem to respond to reading Feeling Good, it is also clear that some patients with more severe or chronic depressions will need the help of a therapist and possibly an antidepressant medication as well. p. xxviii
One or two studies are hardly conclusive, but these were promising findings. More recently, several studies have been conducted on the effectiveness of other self-help manuals. For the most part, the findings are similar to the studies from the 1990s cited by Burns. According to a 2007 Wall Street Journal article(subscription required), bibliotherapy is most effective when used in conjunction with other forms of therapy.
Cognitive Behavioral Therapy

Feeling Good and most of the popular self-help workbooks use the model of Cognitive Behavioral Therapy (CBT). This approach helps you identify specific patterns of thinking that support a negative view of yourself and reinforce the emotional lows of depression. The method teaches you to counteract these habitual patterns with more realistic ones so that your mind opens to a balanced interpretation of experience rather than one that is always negative.
CBT techniques lend themselves especially well to working on your own. Many therapists either provide worksheets for daily practice or recommend the use of workbooks that include blank forms in which you can note these patterns and then write your own words to counteract them.
I would imagine, then, that the benefit of workbooks comes not just from reading but also from interacting with the content and practicing new skills. For me, both the reading and writing have helped a lot because I find there’s a powerful restorative effect from formulating words and concepts to pinpoint what I’m experiencing.
Reading and Neuroplasticity
There doesn’t seem to be a lot of research about why bibliotherapy works, but I’ve run into untested ideas that relate the process of reading to the recent emphasis on neural plasticity. That’s the ability of the brain to form new neural circuits and activate areas of the brain that haven’t been functioning well. The concept is that learning by reading helps form new circuits that can change habitual thought patterns. By introducing new possibilities and neural connections, parts of the brain that are less, or more, active under the influence of depression can be restored to a the patterns of non-depressed brains.
But whatever might be going on with the brain, I know I’ve felt more hope for recovery and made progress on my own by reading books – and, just as important, reading blogs and other online sources of information. The process of absorbing new ideas through the impact of written words can be helpful whether or not you like to use workbooks and practice exercises.
Written by: John Folk-Williams, Storied Mind,
Twitter: @StoriedMind
The views of the article and writer and are not expressly the views of Exult Healthcare, although Exult Healthcare has consulted the author for use and proper attribution of the article.
Looking Under the Shadows
During severe depression something people take solace in the idea that they could end it all but a majority of people never act upon it due to religious views, support systems, family commitments or the knowledge that the depression will pass. Sometimes the emotional pain becomes seemingly so unbearable the idea of suicide leads to action.
Normally, the person thinks family members would be better off without them because they are a burden. The depression feeds into negative thoughts that feel like truths like “you are worthless” or “you will never amount to anything”. They can not see beyond the reality that the depression is projecting. The current depression is all consuming and the future looks like a dystopia.
A person with severe depression usually isolates themselves to the point that they feel there is no one to turn too.
They have anhedonia, a loss of pleasure in things and activities, so what normally would make them happy and pull them out of the depression. They loss the ability to concentrate and the world is just a blur and they are unable to make logical and informed decisions. They are afraid to ask for help or are embarrassed that they cannot cope with things on their own. The darkness seems for engulfing that they can not look up to see the sun. The all-encompassing nature of depression makes it hard to untangle from it on their own.
Some Warning Signs of a Pending Attempt:
- feeling hopeless
- feeling intolerable emotional pain related to depression
- having an abnormal fascination w/ death and dying or talking about suicide or dying
- having mood swings from happy to sad
- increased irritability
- talking about issues related to anger, guilt or shame
- have an increase in anxiety
- experiencing changes in personality, routine, or sleeping patterns
- Decrease in hygiene
- Unable to get out of bed
- personality changes
- an increase or recent usage of drugs and alcohol
- engaging in risky behavior that could lead to an accidental death
- putting their affairs in order like giving away important possessions
- resolving issues or staying goodbye to people
- gathering means to commit suicide
- increased isolation
- feeling they are a burden to others
- seeming to be unable to experience pleasurable emotions from normally pleasurable activities
- negative thoughts like “I’m useless.” or “Everyone would be better off if I was not here.”
- relationship issues
- bullying
- trauma
Please seek help, if you or someone you know is suicidal. Assistance can be provided at your local ER or mental health facility.
The National Suicide Prevention Lifeline is always open. You can reach a trained counselor at 800-273-TALK (800-273-8255) or chat online at https://suicidepreventionlifeline.org/
Text the Crisis Support line at 741741
Written by: Karen Limme, LPC-Intern
Eating away a Disorder
According to the CDC almost 40% of adults over the age of 20 are considered obese. Obesity is defined as having a body mass index (BMI) of 30 and above. Obesity remains the leading cause of heart disease, diabetes and certain types of cancer. For many, weight gain is a result of medical issues or a side effect of medications.
 For others it could be due to disordered eating behaviors that include stress eating, eating when full, eating in secret or feeling loss of control while eating. Emotional eating is the act of using food to satisfy one’s emotional needs rather than to satisfy hunger. Most people identify as emotional eaters, after all, who hasn’t come home from a hard day at work and wanted to eat pizza or sat down with a pint of ice cream after a break-up?
For others it could be due to disordered eating behaviors that include stress eating, eating when full, eating in secret or feeling loss of control while eating. Emotional eating is the act of using food to satisfy one’s emotional needs rather than to satisfy hunger. Most people identify as emotional eaters, after all, who hasn’t come home from a hard day at work and wanted to eat pizza or sat down with a pint of ice cream after a break-up?
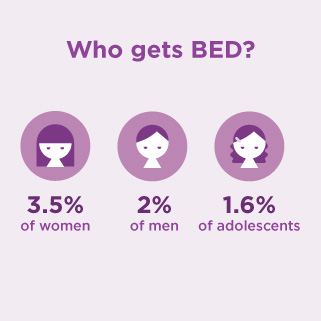
Although this might sound like binge eating, it is very different from an actual diagnosis of Binge Eating Disorder (BED). BED is characterized by out of control eating that occurs frequently, is out of control and leaves a person with intense feelings of guilt and shame. BED occurs when a person eating an amount of food not normal for them in one sitting, at least twice a month.

In a binge episode, people tend of eat thousands of calories of highly processed foods (e.g. pizza, fast food, ice cream, candy, cookies), rapidly, in secret and until they are uncomfortably full (even then some). People tend to use the term “binge” to describe over eating, but BED is an eating disorder that needs to be addressed by a multidimensional team of professionals like a medical doctor, dietitian and a therapist.
Written by Cynthia D’Sauza,
Clinical Director, LPC, LMFT, PhD
BED-7 Test ( This test is a diagnostic and does not reflect Exult’s view)
1. During the last 3 months, did you have any episodes of excessive overeating?
2. Do you feel distressed about your episodes of excessive overeating?
3. During your episodes of excessive overeating, how often did you feel like you had no control over your eating?
4. During your episodes of excessive overeating, how often did you continue eating even though you were not hungry?
5. During your episodes of excessive overeating, how often were you embarrassed by how much you ate?
6. During your episodes of excessive overeating, how often did you feel disgusted with yourself or guilty afterward?
7. During the last 3 months, how often did you make yourself vomit as a means to control your weight or shape?